When you’re experiencing excruciating back pain, it overtakes your entire life. Every waking moment you’re reminded by the pulsating pain that just doesn’t seem to go away. As a last resort, you turn to epidural steroid injections – but the pain gets worse.
But wait, aren’t steroid injections that your doctor enthusiastically recommended supposed to make the pain go away? Not necessarily.
Unfortunately, many people who experience intense back and neck pain are left with little to no other options. That is, if they turn to their medical doctors for help managing the pain. When it comes to back pain, medical doctors often recommend pain-killers like ibuprofen, or prescription-only NSAIDs like diclofenac (Voltaren), or celecoxib (Celebrex). If those don’t work, they’ll often recommend epidural steroid injections, which come with some terrifying risks.
What Are Epidural Steroid Injections
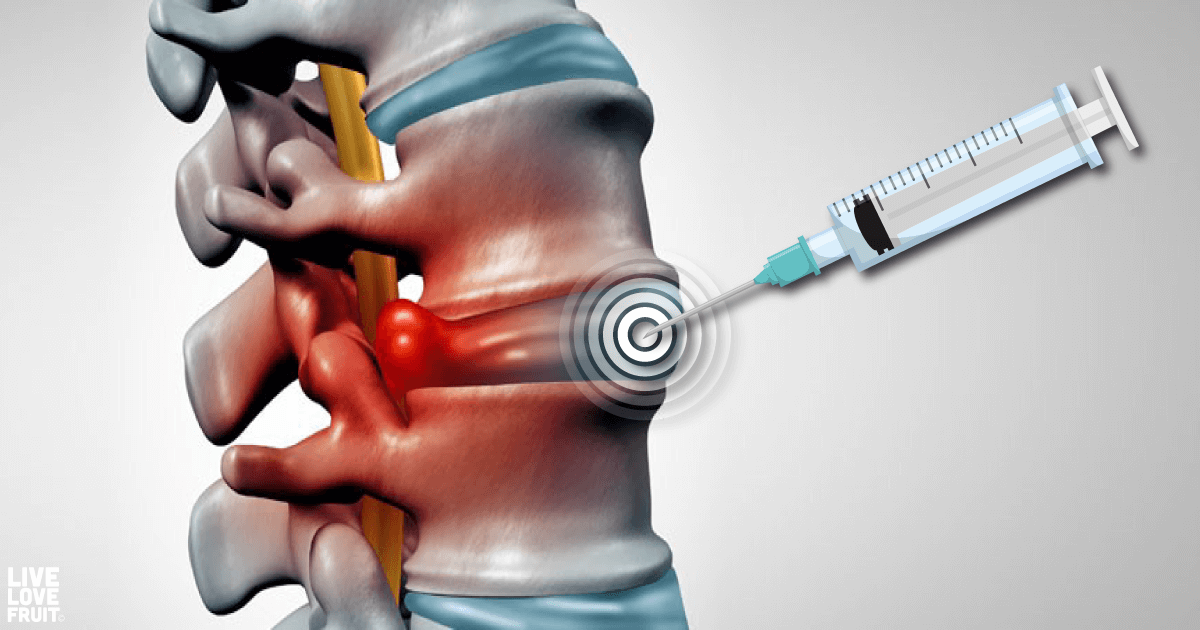
Epidural steroid injections are a treatment option commonly used for low back and leg pain. They have been used for low back problems since the early 1950’s, and are currently used for non-surgical management of sciatica and low back pain (1).
To help a patient relieve spinal pain, a doctor will inject the epidural space (between the spinal cord and bony structure of the spine) with steroids.
The injection usually consists of (2):
– Steroids or cortisone (anti-inflammatory agent)
– Lidocaine (fast-acting local anesthetic)
– Saline (dilutes local anesthetic)
Once the steroids are injected, the mixture is supposed to have an anti-inflammatory effect that can last anywhere from a few days to a few months (3).
Unfortunately, the epidural space is a very delicate part of the body, making the procedure extremely risky.
The Risks of Epidural Steroid Injections
In April 2014, the U.S. Food and Drug Administration (FDA) issued a drug safety communication entitled “FDA requires label changes to warn of rare but serious neurologic problems after epidural corticosteroid injections (ESI) for pain (4).” The FDA’s warning even stated that they could “result in rare but serious adverse events, including loss of vision, stroke, paralysis, and death (5).”
The side effects of epidural steroid injections are so severe that the FDA ruled that all injectable steroid must carry an updated warning that includes the above risks, as well as “arachnoiditis, bowel/bladder dysfunction, headache, meningitis, paraparesis/paraplegia, seizure, [and] sensory disturbances (6).”
The FDA’s website also warns that “the effectiveness and safety of injection of corticosteroids into the epidural space of the spine have not been established, and FDA has not approved corticosteroids for this use (7).” This is largely due to the fact that research into the risks of epidural steroid injections is still being conducted. Approved or not, Dennis Capolongo of the ENDC, a ground that has campaigned against epidural steroid injections for years, believes that warning labels need to be stronger, and more visible – not just confined to the small print.
Australia and New Zealand updated their warnings in February 2018, such that steroid injections “MUST NOT be used by the intrathecal, epidural, intravenous or any other unspecified routes (8).” Unfortunately, this isn’t the case for corticosteroid injections in the USA, as doctors still use them for purposes that carry much too heavy of a risk.
In a forum on SPINE-health, one woman with pain in her lumbar spine described her first steroid injection as following:
“I don’t know what went wrong, as was told I’d feel a couple of bee stings, then maybe some pressure. I have a new scale for pain now, and on a scale of 1-10, it was 15. The most excruciating pain I’ve ever experienced. I passed out from it, and my blood pressure dropped to 78/52. They had to give me oxygen, smelling salts, wet towels, etc. They will NEVER do that to me again. Intensely painful and a nightmare.”
Another woman, Helen Bertelli, was diagnosed with arachnoiditis, an incurable condition that can be associated with epidural steroid injections. After her epidural steroid injections for back pain, she started feeling electric shocks, muscle cramps, and a sensation of water running down her legs (9). “I had this feeling I was connected to the end of a guitar string and someone was plucking it. My legs just exploded like there were fireworks in them. My muscles twitched like they were boiling.”
While this pain-relieving procedure may initially provide some relief, the scary symptoms and risks make it not so worth it.
What You Can Do Instead
While seeking medical aid from a doctor is important if your back pain came on suddenly, or if your back pain is so bad that day-to-day life becomes a constant struggle, managing back pain can be much simpler than you think. While it may require a little effort on your behalf, managing back pain doesn’t always have to be remedied with epidural steroid injections.
If you haven’t tried the following suggestions to help remediate your lower back or hip pain, I recommend giving them a try!
Stretch
This one might seem obvious, but I’m serious when I say stretch! Regular stretching helps protect your back by increasing flexibility and decreasing the risk of injury. A lot of people go for epidural injections for sciatica pain to release the sciatic nerve. However, more often than not, the sciatic nerve is being pinched by a tight piriformis muscle, which needs to be released. Check out my article on stretching the piriformis, and if your issue is more back-related, I have tons of articles on stretching out the muscles that trigger tightness in the back muscles.
Eat an Anti-Inflammatory Diet
Consuming an anti-inflammatory diet is crucial if you’re wanting to live pain-free. Many foods have been shown to reduce (or increase) inflammation, a known cause for back pain and inflamed nerves (which epidurals are designed to alleviate). So when you have back pain, changing your diet may help you avoid it.
Eating a mostly plant-based diet, which includes anti-inflammatory foods like chia seeds, broccoli, leafy greens, turmeric, watermelon, and the like, is a great option to help reduce body aches and pains. It is also important to reduce the consumption of foods that cause chronic inflammation in the body like wheat, refined sugar, trans fats, conventional meats, dairy and vegetable and seed oils.
Also, don’t forget to drink enough water! Drinking 3-4 liters a day will ensure you’re flushing out all the acidic waste deposits that contribute to body pain.
Essential Oils
Utilizing pain-relieving essential oils in your day-to-day regimen to alleviate different aches and pains is actually more effective than you might think. Studies have found that applying essential oils on the skin allow their natural components to absorb into the bloodstream (10). So while you may think that putting essential oils on the skin and area of pain is pointless, it actually really works (I can attest to this myself!).
One of my favorite pain-relieving essential oils is copaiba essential oil, which contains the cannabinoid beat-caryphyllene (BCP). It specifically targets CB2 receptors, which aid in the reduction of inflammation and pain.
Other pain-relieving essential oils include things like rosemary, frankincense, myrrh and spruce.
Prolotherapy
Prolotherapy is a natural, alternative therapy, also known as regenerative joint injection or non-surgical ligament and tendon reconstruction. Prolotherapy is a procedure whereby a natural irritant is injected into the soft tissue of an injured joint or spine, which then kick-starts the body’s healing response. Prolotherapy can be expensive, but the results, according to many, are very worth it.





I have medicare , they pay for injection , why do they pay if its not FDA approved?
As described in the article, the medical system gets around it. It is still allowed, even though the FDA warns of the dangers.
Carly, I developed a stenosis in my left lower lumbar region. It also rather abruptly caused my left leg/foot to not function properly (foot drop). I have adopted most of the recommendations to reduce over inflammation however my spine MD is recommending a cortisone epidural. I can manage the lower lumbar pain myself but the left leg dysfunction is not improving. Do you think the epidural will help that condition? If not, any advice?
Sorry, but this is far beyond my scope. I’d recommend seeing a physiotherapist or manual osteopathic practitioner.
Mike, for what’s it worth, there are no peer reviewed studies in the Medical Literature that proves ESI’s are efficacious for spinal stenosis. In fact there are plenty of studies that claim the exact opposite. Look up papers and studies by a Dr. Janna Friedly (Chief of Rehabilitation Medicine / U. Washington Medical Center and FDA/CDER consultant) One more thing, The American Association of Anesthesiology (ASA) have warned that ESI therapy should only be reserved for certain Acute Sciatica cases, with emphasis on “Acute”. Even then the ASA admits its not a permanent fix only a temporary short term patch until further corrective action is performed. ESI’s were never meant to be used as a “Maintenance Therapy” either. Both the ASA and Pfizer have warned of the dangers claiming ESI’s “should never be considered a cure or substitute for when corrective surgery is required”. Dr. Friedly also testified that ESI’s have never shown they reduce the need for surgical intervention, and in fact evidence now points to the exact opposite, ESI can even produce false negative results (exacerbating symptoms) needlessly confusing doctors and thus promoting the need for unnecessary surgeries.
Thanks for the informative and clear comments, Dennis. I greatly appreciate it.
I think the point of this article we all just read is : “stay away from epidurals”
Prolo therapy was mentioned. By the very nature of what it does be prepaired for immense pain. It worked for me for awhile but it was the most pain I’ve ever expeienced in my life.
Yes Carly is 100% correct! Unfortunately the system is rigged in favor of the medical industry. The FDA does not regulate the “practice of medicine”, just the products (drugs and devices) the industry uses. Even then doctors are free to practice medicine how they see fit here in the USA. In fact doctors can inject “gasoline” (no exaggeration) if they wish as long as they obtain a signed “Consent” form from the patient. It’s that simple. Heck, back in 2012, Medicare (CMS) didn’t even know ESI’s were not FDA approved until we told them so. Boy did their faces turn pale with embarrassment.
How long after a back injection can someone have negative side effects? Can it be weeks after?
I had my first L 5 back injection on Oct 29 and began having transient stiffness in my upper back starting the following week. Then, last Friday November 13, my back stiffness became more intense – it lasted through to the following Tuesday. I woke up with a horrific headache I couldn’t explain that lasted the greater part of the day on Wednesday the 19th. I was so nauseous and ultimately ended up throwing up. This has never happened to me before. I have been nauseous ever since. I do not have a fever but have noticed a great increase in thirst after the first injection.
I tried to explain the stiffness to my dr and he shrugged it off. I am worried this may continue into my next session and become worse. ( I have to have 2 epidurals before they ultimately do ablation) Have you heard of this as a side effect and what advice if any can you lend? Thank you!
Yes, it can happen weeks after. I would search out a physiotherapist or osteopathic manual practitioner.
Kate, the post injection symptoms you describe can be serious and should have been reported immediately to the doctor who injected you. Your discharge papers should have made this clear as mandated by law. These new symptoms require an independent evaluation by a second opinion doctor outside your injectionists’ network. Time is important here. First, your post injection headache, especially if its severe enough is a clear indicator of a spinal puncture, where the injectionist accidentally punches a hole in your spinal cord causing the Cerebral Spinal Fluid (CSF) to gush out. This is called Intracranial Hypotension causing low pressure in the skull and spine cord. If not treated with a blood-patch, it could lead to serious future health issues. Second, any who in your spinal cord will allow the steroid, anesthetic and or your own blood to enter the spinal cord and cause future complications such as Leptomeningitis and even Arachnoiditis. You should know that ESI’s are NOT FDA approved for safety and efficacy. In fact, back in 2014 steroid manufactures along with the FDA have issued new warnings that state ESI’s are very risky and worthless with little to no effect on the cause of the underlining cause of the inflammation. The nausea & stiffness you report are also a very bad sign. Is this a Workers Comp case or your Insurance providers mandate before they will authorize and pay for surgical intervention? You may wish to reach out to The EDNC, a patient advocacy group in Washington DC that represents victims of botched ESI’s for more information.
Hello Dennis,
Thank you for your response. The headache did not occur immediately after the injection. Rather, it occurred two weeks after. So I’m not sure if that would indicate a puncture situation. The spasms and stiffness started approximately a week after, and continue to do so now.
The Dr’s assistant told me two ESIs are required by my insurance company before they can move forward with any other kind of treatment. The next step after that is nerve root ablation. Not sure I want that done, but that is the route they say we have to take. They even said they knew ESIs are not effective but they were not given any other choice by my insurance. I am still waiting for a call back from their office.
I had a lower epidural at my L3 and as soon as he put the medicine in my vagina started burning and it felt like I was peeing but I wasn’t like a water flow. I have had a bad headache that will not go away since.
Wow, yeah the effects of this stuff aren’t pretty 🙁
Yes, since ESI’s were never FDA approved the data on procedural mistakes are still being compiled. But based on your comment, I would say you are suffering from a Dura puncture (the membrane covering your spinal cord) that surrounds the all your spinal nerves. This mistake can cause a Cerebral Spinal Fluid leak (CSF Leak). This usually indicates the physician went too far with the ESI needle. These leaks cause severe headaches, lightheadedness, even ataxia, photophobia, etc and can be very difficult to plug up once they happen. The flip side can be even worse, the doctor not only went too far with the needle, he accidentally injected the steroid mixture into your CSF or allowed blood enter your CSF through that puncture. These are all serious mistakes.
So please report such issues directly to your PCP as soon as possible especially if you develop bladder & bowel dysfunction, chronic headaches & migraine, increased pain symptoms or new pain centers and symptoms. You may need expert intervention. BTW, a blood patch is not always the best solution if the CSF leak doesn’t resolve on its own. Wishing you the best.